
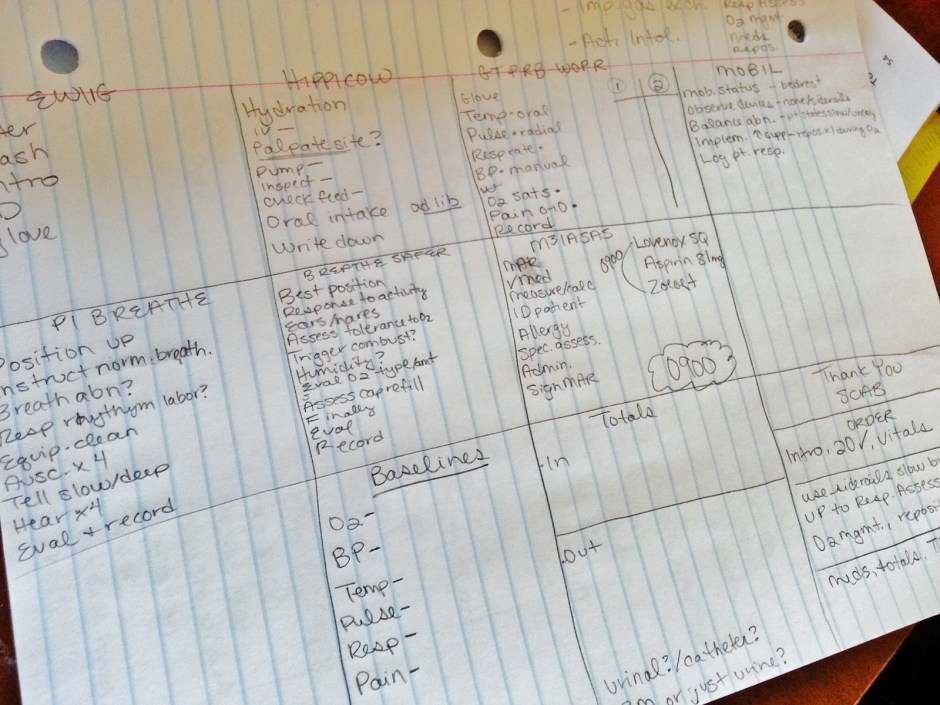
Here are my careplans written verbatim (at least as best as I can remember) and my PCS Kardex info and AOC’s. I was able to use activity intolerance with all three patients and believe that this is highly likely for anyone’s weekend, so I’d remember to think of that one first every time and see if it can fit before trying to think up something else.
The way I wrote my care plans was to look immediately at the areas of care assigned, based on that I started to think of my priority diagnosis- the important one and highest ranked according to Maslow’s. So I immediately looked and sorted info in my head- Airway, Breathing, Circulation, Pain. I didn’t even look at their admitting diagnosis, or any other relevant info until I had perused the AOC’s and had my priority, then I’d use the other info to validate my choice (this is where my AEB came from).
So for example I look down at the Kardex- I have oxygen management and they are indeed on oxygen, I immediately think Impaired Gas Exchange, then I look up to their admitting diagnosis which says pneumonia- BINGO, we’re good. Impaired Gas Exchange r/t ventilation perfusion imbalance aeb dyspnea. If I was unsure about any of the r/t or aeb I would just leave it off until I had a chance to either check the chart to be sure or get report from primary to validate.
***For my priority picks I NEVER continued to use a label without perfect evidence of the r/t and aeb because I knew that this would be the diagnosis that I’d use for my evaluation and I would HAVE to have this info, if I wasn’t 1 million percent sure I didn’t go with it***
That being said for my second pick I would go with something that would work and if I didn’t have clear evidence of an r/t or aeb I’d just leave that off of the planning care plan (it’s not required there anyway). AND I would pick an outcome that fit the diagnosis even if I didn’t know or really think that my patient would be able to achieve it. I did this because you don’t have to rationalize your outcome or interventions for your second pick, ONLY the first, so who cares if they didn’t meet the outcome or if they refused your intervention! Chart it and who cares, it’s only the first pick that I wanted to be sure was bulletproof, that had interventions that I could get in without problem, that had an outcome I could easily meet. Because by doing this I avoided revisions and avoided the dreaded thought of marking the “unmet” or “ineffective” boxes on the evaluation. I didn’t want to open the door for ANYTHING there that could fail me.
Along the same lines I worded my interventions in a way that I would be able to complete them with or without patient cooperation for the most part, again avoiding revisions. For example “Encourage patient to use controlled breathing techniques during ambulation” instead of putting “Nurse will have patient use controlled breathing” because if your patient says no or doesn’t do it you have to revise. Same with outcomes to an extent- “Patient will participate in ambulation without complaints of dyspnea” instead of saying “Patient wont have dyspnea” because it’s easier to lead the patient with what you want them to say “you feel good right? you didn’t seem to have any trouble breathing with that, that’s great huh!” “Much stronger than last time right?” You can’t argue with subjective information when it comes from the patient, if they say they’re good then they’re good. I figured this was a safer way to do things to pass…
I picked every outcome, related to, intervention, and as evidenced by DIRECTLY from the Mosby’s book. You are only required to use the label verbatim but I picked every single thing straight from the book so that there was no way the CE could look at me and say “show me where this intervention is under that label??” Even if the intervention was completely appropriate, if it wasn’t in the book I didn’t even try it. I did pick appropriate interventions, outcomes, and things that fit that particular patient so that I was still specific to the patient but I used the book exactly.
For example: One of the interventions for Activity Intolerance is (pg.169 3rd edition) “Instruct and assist a COPD client in using conscious controlled breathing techniques during exercise including pursed lip breathing” So for my patient that had COPD I went with this. For my patient with the hernia who also had activity intolerance I did NOT use this, since it was mentioned specifically in connection with COPD. Sure that intervention could work with her too, breathing slowly, controlled, etc but she didn’t have COPD so I didn’t use that one. That was my rationale for taking the precise interventions and tailoring them to my specific patient.
****HIGHLIGHT YOUR BOOK with your go-to typical defining characteristics (aeb’s), related factors (r/t’s) and interventions. You don’t have to highlight them all, just the ones that you can expect to see frequently. This will save you precious time in planning!****
PCS #1:
-History of COPD, re-admitted after just being released 2 days ago with pneumonia, complaints of dyspnea.
-Areas of Care Assigned: Vitals, Intake & Output, Fluid Management (with IV access but no IV fluids present), Respiratory assessment, Oxygen management (on 2L/min NC), Medications 0900 (Lovenox, Prozac, Aspirin), Mobility: ambulate hallway.
Dx #1: Impaired Gas Exchange R/T ventilation perfusion imbalance: COPD (including COPD made this part patient specific) AEB patient complaints of dyspnea and fatigue (this was all charted & reported from primary so I knew I was good for eval)
Outcome: Patient will have a capillary refill of less than 3 seconds in both hands during PCS. (I chose cap refill instead of 02 sats because the CE didn’t check 02 sats under oxygen management, it was checked under vitals and I wasn’t sure if I could use it or not in management, so I went with cap refill instead to be on the safe side).
Assessment: Assess patient’s capillary refill in both hands during PCS.
Intervention #1: Nurse will continue to administer oxygen as ordered via nasal canula during PCS. (pg.389) *Notice I didn’t say oxygen at 2L/min because his orders kept changing and I didn’t want to revise, so I changed the wording.
Intervention #2: Nurse will offer rest periods during ambulation during PCS. (pg.390) *Notice I said OFFER, so even if they decline I still did my intervention.
Dx #2: Activity Intolerance R/T imbalance between oxygen supply & demand AEB complaints of exertional dyspnea and fatigue (I could’ve left these off but I had report of them so I included them)
Outcome: Patient will participate in ambulation with no complaints of dyspnea during PCS. *Notice I took what Mosby lists for an outcome and worded it to fit that patient. (I didn’t care if he ended up complaining of dyspnea because I wasn’t evaluating this label as my priority, and obviously he had a bit MORE than just dyspnea during the PCS ha!)
Assessment: Assess patient for signs and complaints of dyspnea during ambulation during PCS. *Putting ‘signs AND complaints’ allowed me flexibility to get objective AND subjective info, more options for charting and/or eval if you need it
Intervention #1: Nurse will instruct patient to move slowly with activity and during ambulation during PCS. (This was my version of “slow the pace of care. Allow the client extra time to carry out physical activities” pg. 169).
Intervention #2: Nurse will encourage patient to use controlled breathing techniques during activity and ambulation during PCS. (pg. 169).
***Notice that most of my interventions literally require me to simply SAY something “hey you should go slow, try and take deep breaths before doing any activity”, this means it will take you seconds to complete and you can be off and running (or your patient can start running 😉 Be conscious of your time the WHOLE time by thinking this through ahead of time***
PCS #2
Recent post op abdominal surgery, hernia repair with extensive adhesions. Was having trouble with pain but not so much once I got to her. JP drains, 2 IV’s running fluids & meds, oxygen @ 2L/min, PCA pump, epidural pump, foley, SCD’s, abdominal binder. Had been having major issue with hypotension (90/50). Overweight but otherwise pretty healthy.
Areas of Care Assigned: Vitals, I & O, Fluid management, Respiratory management with I/S x10, abdominal assessment, pain management, drainage for JPs, mobility: out of bed to chair
*I immediately wanted to hit my “airway” priority and saw respiratory management, but had nothing else relevant, she had no history of breathing issues, and no other risk type issues so that was out even though she was on 02 I was NOT assigned oxygen management. No circulation even though I could’ve stretched for tissue perfusion issues with tissue trauma but I knew that was a bad idea and I wasn’t assigned a PVA. So next priority was pain which I WAS assigned.*
Dx #1: Acute pain R/T tissue trauma: abdominal surgery AEB patient states pain level 4/10 (I was not crazy about using this one since she wasn’t rating her pain very high over the past couple of readings, BUT she had a PCA pump AND an epidural and acute pain was relevant for being newly post op so I ran with it).
Outcome: Patient will rate pain level 3 or less on 0-10 scale during PCS.
Assessment: Assess patients pain level on 0-10 scale during PCS.
Intervention #1: Encourage patient to use PCA pump at regular intervals to better manage pain during PCS. (pg. 550)
Intervention #2: Reposition patient out of bed to chair x1 during PCS.
Dx #2: Activity Intolerance (I left off the R/T since I didn’t have a crystal clear picture, I could’ve probably put imbalance between 02 supply & demand but didn’t chance it). I also left off the AEB even though I knew she had hypotension because this wasn’t my priority dx and I didn’t put it unless I was 200% sure.
Outcome: Patient will participate in transfer out of bed to chair with no signs of hypotension *Notice I used hypotension for her since I knew this was a problem she was having, making it patient specific.
Assessment: Assess patient for signs of hypotension and complaints of dizziness during transfer out of bed to chair.
Intervention #1: Nurse will instruct patient to sit and dangle at the bedside prior to activity and transfer out of bed to chair (pg. 167). *This is not only appropriate for transferring any patient to chair but is mainly to help with orthostatic hypotension, the precise problem she’d been having (patient specific).
Intervention #2: Nurse will offer rest periods during care activities and transfer out of bed to chair during PCS. (I could’ve used reposition out of bed to chair as an intervention which would count as “mobilizing the patient as soon as possible” pg. 166, or “position client upright several times daily” pg. 166 but I had used this intervention for pain and didn’t want to chance it.)
PCS #3
Admitted with severe dyspnea, history of CHF, COPD, diabetes, lupus, depression, and a few other random things.
Areas of Care Assigned: Vitals, Intake & Output, Fluid Management (she had an IVAD but no fluids currently running), Medications 0900 (Prozac, Lasix, Amlodopine, Lovenox, Mucinex), Flush IVAD, Peripheral assessment lower, Mobility- out of bed to chair, Patient teaching with fluid management.
*I had my airway priority obviously with 02, could’ve tried to use tissue perfusion problems for circulation with the PVA and diabetes but I no supporting data so I steered clear (good thing too because she was fine in that department!)*
Dx #1: Impaired Gas Exchange R/T ventillation perfusion imbalance: COPD AEB: patient complaints of severe dyspnea (sound familiar?? Don‘t re-invent the wheel, same problem same history, same diagnosis even on different patient)
Outcome: Patient will have an oxygen saturation of 92% or higher on oxygen during PCS. *I used 02 sats this time since it was checked off under oxygen management this time.
Assessment:Assess patients oxygen saturation on oxygen during PCS.
Intervention #1: Continue to administer oxygen as ordered via NC during PCS.
Intervention #2: Nurse will position patient upright out of bed to chair x1 to facilitate oxygenation during PCS (pg. 388). (I included the tidbit about facilitating oxygen so she knew I was using positioning to help oxygenation, not just positioning for the heck of it).
Dx #2: Activity Intolerance R/T imbalance between oxygen supply and demand (duh, that’s why they have her on oxygen) AEB exertional dyspnea and fatigue (this was reported by primary)
Outcome: Patient will participate in transfer out of bed to chair without signs or complaints of dyspnea. (once again, didn’t care if she ended up having dsypnea since I wasn’t evaluating this one, plus I could probably get her to report an improvement in the dyspnea at the very least if I led the questioning the right way)
Assessment: Assess patient for signs and complaints of dyspnea during transfer out of bed to chair.
Intervention #1: Nurse will instruct patient to sit and dangle prior to transfer out of bed to chair (pg. 167).
Intervention #2: Nurse will encourage patient to move slowly and use controlled breathing during activity and during transfer out of bed to chair (pg. 169)
This is part of my post series on Excelsior College’s ADN nursing program and the CPNE experience. See all related posts over here.
The info presented and/or pictures contain copyrighted content from Excelsior College that may be confidential in nature, this information is meant for demonstrative purposes. No replication of this information is permitted.


One thought on “CPNE Careplans”